Introduction: Erectile dysfunction (ED) is defined as persistent inability to achieve and sustain an erection sufficient for satisfactory sexual performance. The prevalence of ED increases with aging from 9% in men younger than 40 years to 71% in older men. ED impacts negatively on sexual performance and quality of life (QoL). Low-intensity shockwave therapy (LiSWT) for ED is a regenerative therapy and contrary to other current therapeutic options which are mainly palliative, it restores the erectile mechanism enabling natural or spontaneous erections. LiSWT has found significant usefulness in the treatment of ED with potential to induce angiogenesis and dislodge plaques which will invariably improve blood flood to the penis leading to a lifelong solution to ED with marked improvement in sexual performance. Methodology: This is a prospective randomized study. All patients presenting to andrology clinic with erectile dysfunction were enrolled in the study. Informed consent was obtained. All patients were evaluated to identify the likely etiology and a proforma and standard abridged version of International Index of Erectile Function (IIEF-5) were administered. An Emshock and Smart Tecar 2 in 1 device was used to deliver low intensity shockwave to the penis at 5 different sites and treatment sustained twice a week for 3 weeks to complete a cycle before reassessment with IIEF-5 questionnaire. Data obtained were analyzed using Statistical Package for Social Sciences version 22.0. Results were represented in charts. P value of less than 0.005 was considered statistically significant. Results: Fifty four patients were enrolled in the study. The enrolled patients fell within the age ranges of 34 to 63 years. The identifiable etiology of ED were unknown in 22.22%, diabetes mellitus in 46.30%, hypertension in 18.52% and a combination of hypertension and diabetes in 13%. All patient enrolled for the study had varying degree of abnormal IIEF-5 score. Twelve patients (22.22%) had mild ED, eleven patients (20.37%) had mild to moderate ED, one patient (1.85%) had moderate ED and thirty patients (55.56%) had severe ED. All patients had varying significant improvement in erectile function and IIEF-5 score after the first treatment cycle. Eighteen patients (33.33%) achieved normal erection evidenced by progression to normal IIEF-5 while 36 patients (66.66%) achieved significant progress evidenced by improvement in IIEF-5 score. 4 patients had spontaneous erection that lasted more than 20 minutes during each treatment encounter. No patient had side effect and the patient satisfaction was one hundred percent. Conclusion: LiSWT remains revolutionary as a regenerative therapy for restoration to physiological erectile function possibly possessing unprecedented qualities that can rehabilitate erectile tissue. While results of several studies are variable, one thing that is found across many literatures is the low risk and lack of side effects of LiSWT. Its main benefit is the ability to support and potentially restore erectile function in men with ED without additional pharmacotherapy.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Erectile Dysfunction, Low Intensity Shockwave Therapy, International Index of Erectile Function-5, Quality of Life
1. Introduction
Erectile dysfunction (ED) is defined as persistent difficulty or inability to achieve and sustain an erection sufficient for satisfactory sexual performance.
[1]
Obiatuegwu K, Atim T, Magnus F et al. Quadmix Penile Injection: An Initial Urologist Experience. Int J Clin Urol. 2025; 9(1): 73-79.
The prevalence of ED increases with aging from 9% in men younger than 40 years to 71% in older men.
[2]
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6(4): 1103-1110.
The incidence per age distribution shows a rising trend and reported as 31% for men aged 50-59 years to as high as 76% in men above 70 years.
[3]
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47(6): 824-837.
ED impacts negatively on sexual performance and quality of life (QoL) leading to low self-esteem and relationship disharmony.
The most commonly used validated questionnaires for assessment of ED is the 15-item International Index of Erectile Function (IIEF-15) which has been abridged to a 5-item version (IIEF-5) more suited for office use.
[4]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Sexual function assessed by IIEF-5 includes erectile function, orgasmic function, sexual desire, intercourse satisfaction and overall satisfaction. They determine baseline erectile function before commencement of intervention and also assess the progress of specific treatment modality.
Based on IIEF-5, ED is classified as severe (5-7), moderate (8-11), mild to moderate (12-16), mild (17-21), and no ED (22-25).
[4]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Management of ED can be a daunting task and involves a detailed clinical evaluation with targeted investigations including fasting blood sugar, fasting lipid profile, hormonal profile, penile color splash and prostate-specific antigen (PSA) test especially in men above the age of 50.
[1]
Obiatuegwu K, Atim T, Magnus F et al. Quadmix Penile Injection: An Initial Urologist Experience. Int J Clin Urol. 2025; 9(1): 73-79.
Treatment includes lifestyle modification, treatment of comorbid conditions and organic dysfunction, psychosexual therapy, use of medications such as phosphodiesterase type 5 inhibitors (PDE5i), intracavernosal agents such as alprostadil, Bimix, Trimix and Quadmix, penile vacuum device, intraurethral agents, penile implants, penile arterial revascularization and venous ligation surgery and shock wave therapy.
[1]
Obiatuegwu K, Atim T, Magnus F et al. Quadmix Penile Injection: An Initial Urologist Experience. Int J Clin Urol. 2025; 9(1): 73-79.
Low-intensity shockwave therapy (LiSWT) for erectile dysfunction (ED) is becoming increasingly popular in clinical practice as a regenerative therapy with several trials and meta-analysis reporting a favorable outcome with marked improvement in International Index of Erectile Function (IIEF) scores.
[5]
Solomon H, Evan JP, Nelson EB. Variations in low intensity shockwave treatment protocols for erectile dysfunction: A review of literature and guide to offering treatment. World J Mens Health. 2024; 42(2): 283-289.
Available randomized controlled trials and meta-analyses indicate that low-intensity shockwave therapy when compared to sham treatment improves vasculogenic ED by 4 points based on the International Index of Erectile Function- Erectile Function Domain (IIEF-EF).
[6]
Sokolakis I, Hatzichristodoulou G. Clinical studies on low intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic review and meta-analysis of randomised controlled trials. Int J Impot Res. 2019; 31: 177-94.
LiSWT for ED is a regenerative therapy and contrary to other current therapeutic options which are mainly palliative, Li-SWT is unique because it restores the erectile mechanism enabling natural or spontaneous erections.
[7]
ILan G, Boaz A, Noam DK, Yoram V. Shockwave treatment of erectile dysfunction. Ther Adv Urol. 2013; 5(2): 95-99.
There is still discussions and debate over the clinical usefulness of LiSWT and no consensus regarding the optimal treatment protocol has been established. The American Urological Association (AUA) considered LiSWT for ED as investigational (evidence level: grade C) and suggested that the true therapeutic value of LiSWT may differ remarkably from reported outcome.
[8]
Janak Desai, Eric Huyghe, Gayle D Maffulli, Carmen Nussbaum-Krammer, Jessica Tittelmeier, Christoph Schmitz, Extracorporeal shock wave therapy for erectile dysfunction: rethinking study design, implementation, and analysis, British Medical Bulletin, Volume 154, Issue 1, June 2025, ldaf004,
Medications such as PDE5i, topical gels and other non-surgical ED treatments such as intracavernosal injections (ICI), intraurethral suppositories and vacuum erection devices (VED) focus only on palliative symptom management. While these options may be effective and reasonably safe with rare adverse effects, they do not alter the underlying pathophysiology of the erectile mechanism compared to LiSWT. More so, these treatments are usually taken as required and most times prior to the initiation of sexual activity with time bound effect.
[8]
Janak Desai, Eric Huyghe, Gayle D Maffulli, Carmen Nussbaum-Krammer, Jessica Tittelmeier, Christoph Schmitz, Extracorporeal shock wave therapy for erectile dysfunction: rethinking study design, implementation, and analysis, British Medical Bulletin, Volume 154, Issue 1, June 2025, ldaf004,
Low dose tadalafil when administered daily instead of on-demand treatment may improve erectile function but does not restore the physiology of erection. Historically “restorative therapies” have not been well studied though there are emerging favorable data for options like stem cell therapy, platelet rich plasma and low-intensity shockwave therapy (LiSWT). Vardi et al reported their first therapeutic series treating patients with ED in 2010 and marking the introduction of LiSWT for treatment of ED with growing favorable evidence.
[9]
Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol 2010; 58: 243-248.
Technically, shockwave therapy is a clinical intervention which uses sound waves to generate and transmit a positive pressure force on the penis at different points targeting the copora bodies. Shockwave was first applied in the treatment of kidney stones but has now evolved as a popular treatment for other conditions including ED, joint pain, bone pain etc.
[9]
Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol 2010; 58: 243-248.
A shockwave is produced when a wave moves through a surrounding material faster than the speed of sound.
[11]
Katz JE, Clavijo RI, Rizk P, Ramasamy R. The basic physics of waves, soundwaves, and shockwaves for erectile dysfunction. Sex Med Rev 2020; 8: 100-105.
Shockwaves are generated using one of three types of generators viz piezoelectric, electromagnetic or electrohydraulic. Summarily, piezoelectric devices generate a current across piezo crystals causing them to rapidly expand and contract. This causes a pressure pulse that is transmitted through the surrounding water to create a shockwave. Electromagnetic generators use two conflicting magnetic fields to create a wave and an acoustic lens to focus the resulting shockwave while electrohydraulic devices use a high voltage across a capacitor to create a gas bubble. This propagates through the surrounding water and leads to a shockwave that is focused using an acoustic lens.
Katz JE, Clavijo RI, Rizk P, Ramasamy R. The basic physics of waves, soundwaves, and shockwaves for erectile dysfunction. Sex Med Rev 2020; 8: 100-105.
Fode M, Hatzichristodoulou G, Serefoglu EC, Verze P, Albersen M. Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 2017; 14: 593-606.
Extracorporeal shockwave therapy (ESWT) has been clinically investigated and applied in several medical fields with varying rate of success. While high intensity shockwave therapy is used for urinary tract lithotripsy because of its focused mechanical destructive nature, medium intensity shockwaves have been shown to have anti-inflammatory properties and are used for treating varieties of orthopedic conditions such as non-union fractures, tendonitis, and bursitis.
[7]
ILan G, Boaz A, Noam DK, Yoram V. Shockwave treatment of erectile dysfunction. Ther Adv Urol. 2013; 5(2): 95-99.
LiSWT has found significant usefulness in the treatment of ED and is seen as a regenerative therapy with potential to induce angiogenesis and dislodge plaques which will invariably improve blood flood to the penis leading to a lifelong solution to ED with marked improvement in quality of life (QoL) and sexual performance.
[1]
Obiatuegwu K, Atim T, Magnus F et al. Quadmix Penile Injection: An Initial Urologist Experience. Int J Clin Urol. 2025; 9(1): 73-79.
The exact shockwave properties varies depending on the source, however the overall result is a wave that has a sharp onset of peak pressure. There is then a gradual decline in the wave amplitude and a period of negative pressure before the next wave begins.
[11]
Katz JE, Clavijo RI, Rizk P, Ramasamy R. The basic physics of waves, soundwaves, and shockwaves for erectile dysfunction. Sex Med Rev 2020; 8: 100-105.
The cavitation bubble produced by the wave along with mechanical stress from the wave itself transmits force onto the penis when applied to the distal and proximal corpora.
[14]
Sokolakis I, Dimitriadis F, Teo P, Hatzichristodoulou G, Hatzichristou D, Giuliano F. The basic science behind low-intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic scoping review of pre-clinical studies. J Sex Med 2019; 16: 168-194.
[14]
Although the exact mechanism of action of LiSWT for treatment of ED is controversial, conventionally it is believed that shockwaves causes sheer stress on the corporal endothelium leading to neo-angiogenesis, vasodilation and recruitment of stems cells.
[12]
Fode M, Hatzichristodoulou G, Serefoglu EC, Verze P, Albersen M. Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 2017; 14: 593-606.
LiSWT supports and potentially restores erectile function in men with ED without additional pharmacotherapy and seen as a welcoming addition to the armamentarium of existing treatment options for ED.
[7]
ILan G, Boaz A, Noam DK, Yoram V. Shockwave treatment of erectile dysfunction. Ther Adv Urol. 2013; 5(2): 95-99.
LiSWT is a revolutionary treatment of ED and possibly possesses unprecedented qualities that can rehabilitate erectile tissue with consequent return to normal physiology.
[7]
ILan G, Boaz A, Noam DK, Yoram V. Shockwave treatment of erectile dysfunction. Ther Adv Urol. 2013; 5(2): 95-99.
While most reports are variable, LiSWT remains favorable because it poses no risk or side effect compared to other palliative modalities.
[15]
Capogrosso P, Frey A, Jensen C, Rastrelli G, Russo G, Torremade J et al. Low-intensity shock wave therapy in sexual medicine-clinical recommendations from the European Society of Sexual Medicine (ESSM). J Sex Med 2019; 16: 1490-1505.
With appropriate patient selection and counselling regarding cost, benefits as well as long-term efficacy, it is believed that LiSWT is a reasonable and ethical treatment option with a worthwhile anecdotally high patient satisfaction.
2. Methodology
This is a prospective randomized study. All patients presenting to andrology clinic of BeWell Urology and Men’s Clinic Limited Abuja with erectile dysfunction who opted or met the indication for low intensity shockwave therapy were counseled and subsequently enrolled in the study. Informed consent was obtained from those that met the criteria for inclusion.
2.1. Inclusion Criteria
1) Patient with mild, mild to moderate, moderate and severe ED.
2) Patients not responding to medications adequately.
3) Patients not interested in taking medications.
4) Patients that’s desires a regenerative or restorative therapy to reverse ED.
2.2. Exclusion Criteria
1. Patients with ED post radical prostatectomy.
2. Patients with penile implant.
All patients were evaluated to identify the likely etiology and two questionnaires (a proforma and standard abridged version of International Index of Erectile Function -IIEF-5) were administered to all consenting patients to obtain biodata, document the etiology/risk factors as well as objectively assess the severity of ED without bias.
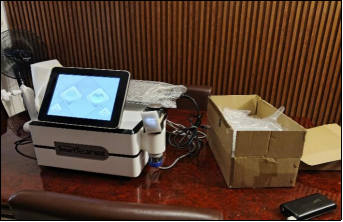
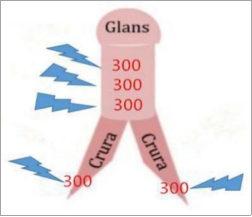
An Emshock and Smart Tecar 2 in 1 device was used to deliver low intensity shockwave to the penis at 5 different sites via the shockwave hand piece as shown in Figures 1 and 2. The spongy tissue is targeted on at least 5 different areas and at least 300 to 500 impacts delivered per area with a total of at least 1500 to 2500 impacts in one treatment as depicted in Figure 3. More impacts was delivered at the top end of the penis and less impacts on the bottom of the penis. The impact was set at a frequency of 8 Hz with energy ranging adjusted between 40 to 80 MJ depending on subsequent response based on review.
Figure 3. Showing 5 different points where the impacts was delivered.
The treatment is sustained twice a week for 3 weeks to complete a cycle before reassessment with IIEF-5 questionnaire and commencement of maintenance cycle if necessary. The erectile function is objectively assessed again at the end of the first treatment cycle using IIEF-5 questionnaire. For the purpose of this study, the erectile function were assessed after the first treatment cycle.
Data obtained were analyzed using Statistical Package for Social Sciences version 22.0. Results were represented in charts. P value of less than 0.005 was considered statistically significant.
3. Results
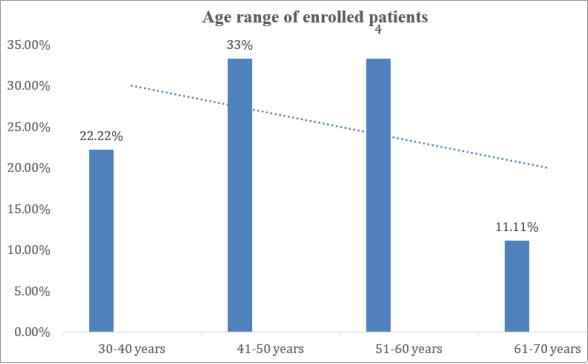
Fifty four patients were enrolled in the study. The enrolled patients fell within the age ranges of 34 to 63 years. Twelve patients (22.22%) were within the age ranges of 30-40 years while eighteen patients (33.33%) were between the age ranges of 41-50 years. Those that fell within the age range of 51-60, and 61-70 years were 33.33% and 11.11% respectively as shown in Figure 4 below.
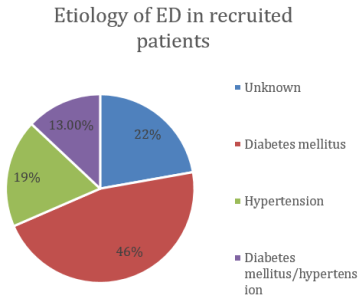
The identifiable etiology of ED in enrolled patients were unknown in 22.22%, diabetes mellitus in 46.30%, hypertension in 18.52% and a combination of both comorbid condition (hypertension and diabetes) in 13% as shown in Figure 5. No patient had trauma, prolonged priapism or any other identifiable organic etiology.
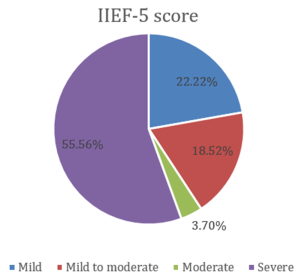
All patient enrolled for the study had abnormal IIEF-5 score. Twelve patients (22.22%) had mild ED, eleven patients (20.37%) had mild to moderate ED, one patient (1.85%) had moderate ED and thirty patients (55.56%) had severe ED as shown in Figure 6.
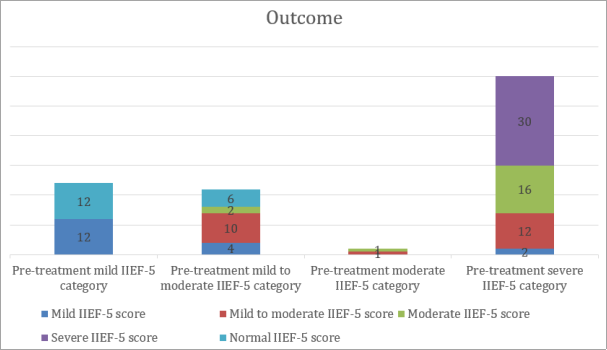
Eighteen patients (33.33%) achieved normal erection evidenced by progression to normal IIEF-5 while 36 patients (66.66%) achieved significant progress evidenced by improvement in IIEF-5 score. 4 patients had spontaneous erection that lasted more than 20 minutes during each treatment encounter. No patient had side effect and the patient satisfaction was one hundred percent.
4. Discussion
Low intensity shockwave therapy (LiSWT) for erectile dysfunction (ED) as a regenerative therapy is becoming increasingly popular in clinical practice with several trials and meta-analysis reporting a favorable outcome with marked improvement in international index of erectile function (IIEF) score.
[5]
Solomon H, Evan JP, Nelson EB. Variations in low intensity shockwave treatment protocols for erectile dysfunction: A review of literature and guide to offering treatment. World J Mens Health. 2024; 42(2): 283-289.
Shockwave therapy is a clinical intervention that employs sound waves to generate and transmit a positive pressure force on the penis at different points targeting majorly the copora bodies.
[9]
Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol 2010; 58: 243-248.
The management of ED has significantly transformed and achieving strong erection has become reasonably simple for some men with ED since the introduction of PDE5i. However PDE5i and most available medical therapy for ED are basically ‘on-demand’ therapies or at best palliative with their mechanism of action targeted at improving a single sexual encounter and this is not without significant untoward effect. Finding a cure or permanent solution to achieving a physiological erection is evolving and low intensity shockwave therapy (LiSWT) is a promising work in progress considering the restorative mechanism of action, ease of administration with little or no side effect.
The age demography in this index study is in keeping with the findings in other studies which reported that ED is commoner in men above the age of 40.
[2]
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6(4): 1103-1110.
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47(6): 824-837.
Fode et al reported that ED affects 30% of all men above the age of 40 with the prevalence exponentially increasing with age. In this study, 77.78% of our patients with ED were above 40 years which confirms that ED is commoner after the age of 40 as reported by several other studies.
[1]
Obiatuegwu K, Atim T, Magnus F et al. Quadmix Penile Injection: An Initial Urologist Experience. Int J Clin Urol. 2025; 9(1): 73-79.
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6(4): 1103-1110.
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47(6): 824-837.
Katz JE, Clavijo RI, Rizk P, Ramasamy R. The basic physics of waves, soundwaves, and shockwaves for erectile dysfunction. Sex Med Rev 2020; 8: 100-105.
Fode M, Hatzichristodoulou G, Serefoglu EC, Verze P, Albersen M. Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 2017; 14: 593-606.
The increased prevalence amongst men above 40 years of age may be due to the presence of comorbid conditions including diabetes mellitus and hypertension, prostate enlargement as well as other organic dysfunction as reported by Obiatuegwu et al. This cormorbid pathologies were also significantly present amongst the participant of this index study.
The etiology of erectile dysfunction in several studies ranges from idiopathic to comorbidities including hypertension and diabetes mellitus, perineal trauma, prostate enlargement, neglected priapism as well as certain medications.
[1]
Obiatuegwu K, Atim T, Magnus F et al. Quadmix Penile Injection: An Initial Urologist Experience. Int J Clin Urol. 2025; 9(1): 73-79.
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6(4): 1103-1110.
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47(6): 824-837.
In this index study, the identified etiology of ED were unknown/idiopathic in 22.22%, diabetes mellitus in 46.30%, hypertension in 18.52% and a combination of both comorbid condition (hypertension and diabetes mellitus) in 13%. The etiology observed in our study is in keeping with documented causes of ED in several studies.
[1]
Obiatuegwu K, Atim T, Magnus F et al. Quadmix Penile Injection: An Initial Urologist Experience. Int J Clin Urol. 2025; 9(1): 73-79.
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6(4): 1103-1110.
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47(6): 824-837.
The presence of prostate enlargement as a contributing factor for ED cannot be over emphasized as majority of the participants were above 40 years of age. This is also in keeping with the finding by Obiatuegwu et al that observed benign prostatic enlargement as the cause of ED in 76.9% of patients.
[4]
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
No patient had perineal trauma and prolonged priapism probably due to the limited sample size.
Ilan et al demonstrated benefits of LiSWT and observed marked progress and improvement in erectile function in 15 men with vasculogenic ED after 4 weeks following LiSWT.
[7]
ILan G, Boaz A, Noam DK, Yoram V. Shockwave treatment of erectile dysfunction. Ther Adv Urol. 2013; 5(2): 95-99.
This is similar to our findings as we observed similar progressive pattern with 33.33% achieving normal erection evidenced by progression to normal IIEF-5 while 66.66% achieved significant progress evidenced by improvement in IIEF-5 score. 22.22% of the patients who achieved normal IIIEF-5 score had spontaneous erection that lasted more than 20 minutes during each treatment encounter. This spontaneous erection during real time intervention with LiSWT may be an indicator of success in patients undergoing regenerative LiSWT. These group of participants were also amongst those that achieved normal IIEF-5. Ilan et al reported a progression by greater than five points in IIEF-5 score in 14 patients while progression by more than 10 points was noted in significant number of patients with an average increase in the IIEF-EF domain scores of 7.4 points (13.5-20.9, p = 0.001). This is similar to our findings in this index study. All our patients had varying significant improvement with erection and IIEF-5 score after the first treatment cycle. Eighteen patients (33.33%) achieved normal erection evidenced by normal IIEF-5 while 36 patients (66.66%) achieved significant progress evidenced by improvement in IIEF-5 score.
Low intensity extracorporeal shockwave therapy (LiSWT) is noninvasive and uses acoustic waves which can pass through the copora bodies to induce angiogenesis and restore natural erectile function.
[12]
Fode M, Hatzichristodoulou G, Serefoglu EC, Verze P, Albersen M. Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 2017; 14: 593-606.
LiSWT remains the only currently marketed restorative therapy for ED which is the most anticipated outcome for most men suffering from ED. Several studies reported no side effect with LiSWT.
[5]
Solomon H, Evan JP, Nelson EB. Variations in low intensity shockwave treatment protocols for erectile dysfunction: A review of literature and guide to offering treatment. World J Mens Health. 2024; 42(2): 283-289.
Sokolakis I, Hatzichristodoulou G. Clinical studies on low intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic review and meta-analysis of randomised controlled trials. Int J Impot Res. 2019; 31: 177-94.
Janak Desai, Eric Huyghe, Gayle D Maffulli, Carmen Nussbaum-Krammer, Jessica Tittelmeier, Christoph Schmitz, Extracorporeal shock wave therapy for erectile dysfunction: rethinking study design, implementation, and analysis, British Medical Bulletin, Volume 154, Issue 1, June 2025, ldaf004,
Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol 2010; 58: 243-248.
Katz JE, Clavijo RI, Rizk P, Ramasamy R. The basic physics of waves, soundwaves, and shockwaves for erectile dysfunction. Sex Med Rev 2020; 8: 100-105.
Fode M, Hatzichristodoulou G, Serefoglu EC, Verze P, Albersen M. Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 2017; 14: 593-606.
This is similar to our findings as no complication was observed in all the patients that participated in the study. Sokolakis et al observed good patient satisfaction with LiSWT. Our study observed similar pattern as all the participants were satisfied with the outcome and opted to continue on maintenance intervention when necessary. All the patients sexual encounter significantly improved and they expressed satisfaction with their QoL and sexual performance.
Despite ongoing debate regarding the efficacy of LiSWT for treatment of ED, LiSWT remains revolutionary as a regenerative therapy for restoration to physiological erectile function possibly possessing unprecedented qualities that can rehabilitate erectile tissue.
[9]
Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol 2010; 58: 243-248.
Katz JE, Clavijo RI, Rizk P, Ramasamy R. The basic physics of waves, soundwaves, and shockwaves for erectile dysfunction. Sex Med Rev 2020; 8: 100-105.
Fode M, Hatzichristodoulou G, Serefoglu EC, Verze P, Albersen M. Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 2017; 14: 593-606.
While results of several studies are variable, one thing that is found across many literatures is the low risk and lack of side effects of LiSWT.
[15]
Capogrosso P, Frey A, Jensen C, Rastrelli G, Russo G, Torremade J et al. Low-intensity shock wave therapy in sexual medicine-clinical recommendations from the European Society of Sexual Medicine (ESSM). J Sex Med 2019; 16: 1490-1505.
With appropriate patient selection and counselling regarding cost, benefits and long-term efficacy, it is believed that LiSWT is a reasonable viable and ethical treatment option with anecdotally high patient satisfaction. Its main benefit is the ability to support and potentially restore erectile function in men with ED without additional pharmacotherapy. We reinstate that LiSWT is a welcome addition to the armamentarium of existing treatment options for ED with promising outcome and little or no side effect.
5. Limitation of the Study
The small sample size may not be a true representation of facts. Future study incorporating other etiologies of erectile dysfunction and possibly involving multiple centers and larger sample size may validate our verdict.
Ethical clearance was obtained from the clinic ethical committee.
Data Availability
All data are in the archive of the clinic record department and readily accessible.
Conflicts of Interest
All the authors declare no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
[1]
Obiatuegwu K, Atim T, Magnus F et al. Quadmix Penile Injection: An Initial Urologist Experience. Int J Clin Urol. 2025; 9(1): 73-79.
Morant S, Bloomfield G, Vat V et al. Increased Sexual Dysfunction in Men with Storage and Voiding Lower Urinary Tract Symptoms. J Sex. Med. 2009; 6(4): 1103-1110.
Raymond C, Francois G and Culley C. Sexual Dysfunction and Lower Urinary Tract Symptoms Associated Benign Prostatic Hyperplasia. European Urol. 2005; 47(6): 824-837.
Kenenna Obiatuegwu, Terkaa Atim, Sadiq Abu et al. Correlation between the Severity of Erectile Dysfunction and Prostate Size in Patients with Benign Prostatic Enlargement. Afr J Urol 27, 31 (2021),
Solomon H, Evan JP, Nelson EB. Variations in low intensity shockwave treatment protocols for erectile dysfunction: A review of literature and guide to offering treatment. World J Mens Health. 2024; 42(2): 283-289.
Sokolakis I, Hatzichristodoulou G. Clinical studies on low intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic review and meta-analysis of randomised controlled trials. Int J Impot Res. 2019; 31: 177-94.
Janak Desai, Eric Huyghe, Gayle D Maffulli, Carmen Nussbaum-Krammer, Jessica Tittelmeier, Christoph Schmitz, Extracorporeal shock wave therapy for erectile dysfunction: rethinking study design, implementation, and analysis, British Medical Bulletin, Volume 154, Issue 1, June 2025, ldaf004,
Vardi Y, Appel B, Jacob G, Massarwi O, Gruenwald I. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month follow-up pilot study in patients with organic erectile dysfunction. Eur Urol 2010; 58: 243-248.
Katz JE, Clavijo RI, Rizk P, Ramasamy R. The basic physics of waves, soundwaves, and shockwaves for erectile dysfunction. Sex Med Rev 2020; 8: 100-105.
Fode M, Hatzichristodoulou G, Serefoglu EC, Verze P, Albersen M. Low-intensity shockwave therapy for erectile dysfunction: is the evidence strong enough? Nat Rev Urol 2017; 14: 593-606.
Sokolakis I, Dimitriadis F, Teo P, Hatzichristodoulou G, Hatzichristou D, Giuliano F. The basic science behind low-intensity extracorporeal shockwave therapy for erectile dysfunction: a systematic scoping review of pre-clinical studies. J Sex Med 2019; 16: 168-194.
[15]
Capogrosso P, Frey A, Jensen C, Rastrelli G, Russo G, Torremade J et al. Low-intensity shock wave therapy in sexual medicine-clinical recommendations from the European Society of Sexual Medicine (ESSM). J Sex Med 2019; 16: 1490-1505.
Kenenna O, Felix M, Terkaa A, Ernest A. Low Intensity Shockwave Therapy for Erectile Dysfunction: Keeping Hope Alive. Advances. 2025;6(4):105-111. doi: 10.11648/j.advances.20250604.11
@article{10.11648/j.advances.20250604.11,
author = {Obiatuegwu Kenenna and Magnus Felix and Atim Terkaa and Aniede Ernest},
title = {Low Intensity Shockwave Therapy for Erectile Dysfunction: Keeping Hope Alive
},
journal = {Advances},
volume = {6},
number = {4},
pages = {105-111},
doi = {10.11648/j.advances.20250604.11},
url = {https://doi.org/10.11648/j.advances.20250604.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.advances.20250604.11},
abstract = {Introduction: Erectile dysfunction (ED) is defined as persistent inability to achieve and sustain an erection sufficient for satisfactory sexual performance. The prevalence of ED increases with aging from 9% in men younger than 40 years to 71% in older men. ED impacts negatively on sexual performance and quality of life (QoL). Low-intensity shockwave therapy (LiSWT) for ED is a regenerative therapy and contrary to other current therapeutic options which are mainly palliative, it restores the erectile mechanism enabling natural or spontaneous erections. LiSWT has found significant usefulness in the treatment of ED with potential to induce angiogenesis and dislodge plaques which will invariably improve blood flood to the penis leading to a lifelong solution to ED with marked improvement in sexual performance. Methodology: This is a prospective randomized study. All patients presenting to andrology clinic with erectile dysfunction were enrolled in the study. Informed consent was obtained. All patients were evaluated to identify the likely etiology and a proforma and standard abridged version of International Index of Erectile Function (IIEF-5) were administered. An Emshock and Smart Tecar 2 in 1 device was used to deliver low intensity shockwave to the penis at 5 different sites and treatment sustained twice a week for 3 weeks to complete a cycle before reassessment with IIEF-5 questionnaire. Data obtained were analyzed using Statistical Package for Social Sciences version 22.0. Results were represented in charts. P value of less than 0.005 was considered statistically significant. Results: Fifty four patients were enrolled in the study. The enrolled patients fell within the age ranges of 34 to 63 years. The identifiable etiology of ED were unknown in 22.22%, diabetes mellitus in 46.30%, hypertension in 18.52% and a combination of hypertension and diabetes in 13%. All patient enrolled for the study had varying degree of abnormal IIEF-5 score. Twelve patients (22.22%) had mild ED, eleven patients (20.37%) had mild to moderate ED, one patient (1.85%) had moderate ED and thirty patients (55.56%) had severe ED. All patients had varying significant improvement in erectile function and IIEF-5 score after the first treatment cycle. Eighteen patients (33.33%) achieved normal erection evidenced by progression to normal IIEF-5 while 36 patients (66.66%) achieved significant progress evidenced by improvement in IIEF-5 score. 4 patients had spontaneous erection that lasted more than 20 minutes during each treatment encounter. No patient had side effect and the patient satisfaction was one hundred percent. Conclusion: LiSWT remains revolutionary as a regenerative therapy for restoration to physiological erectile function possibly possessing unprecedented qualities that can rehabilitate erectile tissue. While results of several studies are variable, one thing that is found across many literatures is the low risk and lack of side effects of LiSWT. Its main benefit is the ability to support and potentially restore erectile function in men with ED without additional pharmacotherapy.
},
year = {2025}
}
TY - JOUR
T1 - Low Intensity Shockwave Therapy for Erectile Dysfunction: Keeping Hope Alive
AU - Obiatuegwu Kenenna
AU - Magnus Felix
AU - Atim Terkaa
AU - Aniede Ernest
Y1 - 2025/10/30
PY - 2025
N1 - https://doi.org/10.11648/j.advances.20250604.11
DO - 10.11648/j.advances.20250604.11
T2 - Advances
JF - Advances
JO - Advances
SP - 105
EP - 111
PB - Science Publishing Group
SN - 2994-7200
UR - https://doi.org/10.11648/j.advances.20250604.11
AB - Introduction: Erectile dysfunction (ED) is defined as persistent inability to achieve and sustain an erection sufficient for satisfactory sexual performance. The prevalence of ED increases with aging from 9% in men younger than 40 years to 71% in older men. ED impacts negatively on sexual performance and quality of life (QoL). Low-intensity shockwave therapy (LiSWT) for ED is a regenerative therapy and contrary to other current therapeutic options which are mainly palliative, it restores the erectile mechanism enabling natural or spontaneous erections. LiSWT has found significant usefulness in the treatment of ED with potential to induce angiogenesis and dislodge plaques which will invariably improve blood flood to the penis leading to a lifelong solution to ED with marked improvement in sexual performance. Methodology: This is a prospective randomized study. All patients presenting to andrology clinic with erectile dysfunction were enrolled in the study. Informed consent was obtained. All patients were evaluated to identify the likely etiology and a proforma and standard abridged version of International Index of Erectile Function (IIEF-5) were administered. An Emshock and Smart Tecar 2 in 1 device was used to deliver low intensity shockwave to the penis at 5 different sites and treatment sustained twice a week for 3 weeks to complete a cycle before reassessment with IIEF-5 questionnaire. Data obtained were analyzed using Statistical Package for Social Sciences version 22.0. Results were represented in charts. P value of less than 0.005 was considered statistically significant. Results: Fifty four patients were enrolled in the study. The enrolled patients fell within the age ranges of 34 to 63 years. The identifiable etiology of ED were unknown in 22.22%, diabetes mellitus in 46.30%, hypertension in 18.52% and a combination of hypertension and diabetes in 13%. All patient enrolled for the study had varying degree of abnormal IIEF-5 score. Twelve patients (22.22%) had mild ED, eleven patients (20.37%) had mild to moderate ED, one patient (1.85%) had moderate ED and thirty patients (55.56%) had severe ED. All patients had varying significant improvement in erectile function and IIEF-5 score after the first treatment cycle. Eighteen patients (33.33%) achieved normal erection evidenced by progression to normal IIEF-5 while 36 patients (66.66%) achieved significant progress evidenced by improvement in IIEF-5 score. 4 patients had spontaneous erection that lasted more than 20 minutes during each treatment encounter. No patient had side effect and the patient satisfaction was one hundred percent. Conclusion: LiSWT remains revolutionary as a regenerative therapy for restoration to physiological erectile function possibly possessing unprecedented qualities that can rehabilitate erectile tissue. While results of several studies are variable, one thing that is found across many literatures is the low risk and lack of side effects of LiSWT. Its main benefit is the ability to support and potentially restore erectile function in men with ED without additional pharmacotherapy.
VL - 6
IS - 4
ER -
Kenenna O, Felix M, Terkaa A, Ernest A. Low Intensity Shockwave Therapy for Erectile Dysfunction: Keeping Hope Alive. Advances. 2025;6(4):105-111. doi: 10.11648/j.advances.20250604.11
@article{10.11648/j.advances.20250604.11,
author = {Obiatuegwu Kenenna and Magnus Felix and Atim Terkaa and Aniede Ernest},
title = {Low Intensity Shockwave Therapy for Erectile Dysfunction: Keeping Hope Alive
},
journal = {Advances},
volume = {6},
number = {4},
pages = {105-111},
doi = {10.11648/j.advances.20250604.11},
url = {https://doi.org/10.11648/j.advances.20250604.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.advances.20250604.11},
abstract = {Introduction: Erectile dysfunction (ED) is defined as persistent inability to achieve and sustain an erection sufficient for satisfactory sexual performance. The prevalence of ED increases with aging from 9% in men younger than 40 years to 71% in older men. ED impacts negatively on sexual performance and quality of life (QoL). Low-intensity shockwave therapy (LiSWT) for ED is a regenerative therapy and contrary to other current therapeutic options which are mainly palliative, it restores the erectile mechanism enabling natural or spontaneous erections. LiSWT has found significant usefulness in the treatment of ED with potential to induce angiogenesis and dislodge plaques which will invariably improve blood flood to the penis leading to a lifelong solution to ED with marked improvement in sexual performance. Methodology: This is a prospective randomized study. All patients presenting to andrology clinic with erectile dysfunction were enrolled in the study. Informed consent was obtained. All patients were evaluated to identify the likely etiology and a proforma and standard abridged version of International Index of Erectile Function (IIEF-5) were administered. An Emshock and Smart Tecar 2 in 1 device was used to deliver low intensity shockwave to the penis at 5 different sites and treatment sustained twice a week for 3 weeks to complete a cycle before reassessment with IIEF-5 questionnaire. Data obtained were analyzed using Statistical Package for Social Sciences version 22.0. Results were represented in charts. P value of less than 0.005 was considered statistically significant. Results: Fifty four patients were enrolled in the study. The enrolled patients fell within the age ranges of 34 to 63 years. The identifiable etiology of ED were unknown in 22.22%, diabetes mellitus in 46.30%, hypertension in 18.52% and a combination of hypertension and diabetes in 13%. All patient enrolled for the study had varying degree of abnormal IIEF-5 score. Twelve patients (22.22%) had mild ED, eleven patients (20.37%) had mild to moderate ED, one patient (1.85%) had moderate ED and thirty patients (55.56%) had severe ED. All patients had varying significant improvement in erectile function and IIEF-5 score after the first treatment cycle. Eighteen patients (33.33%) achieved normal erection evidenced by progression to normal IIEF-5 while 36 patients (66.66%) achieved significant progress evidenced by improvement in IIEF-5 score. 4 patients had spontaneous erection that lasted more than 20 minutes during each treatment encounter. No patient had side effect and the patient satisfaction was one hundred percent. Conclusion: LiSWT remains revolutionary as a regenerative therapy for restoration to physiological erectile function possibly possessing unprecedented qualities that can rehabilitate erectile tissue. While results of several studies are variable, one thing that is found across many literatures is the low risk and lack of side effects of LiSWT. Its main benefit is the ability to support and potentially restore erectile function in men with ED without additional pharmacotherapy.
},
year = {2025}
}
TY - JOUR
T1 - Low Intensity Shockwave Therapy for Erectile Dysfunction: Keeping Hope Alive
AU - Obiatuegwu Kenenna
AU - Magnus Felix
AU - Atim Terkaa
AU - Aniede Ernest
Y1 - 2025/10/30
PY - 2025
N1 - https://doi.org/10.11648/j.advances.20250604.11
DO - 10.11648/j.advances.20250604.11
T2 - Advances
JF - Advances
JO - Advances
SP - 105
EP - 111
PB - Science Publishing Group
SN - 2994-7200
UR - https://doi.org/10.11648/j.advances.20250604.11
AB - Introduction: Erectile dysfunction (ED) is defined as persistent inability to achieve and sustain an erection sufficient for satisfactory sexual performance. The prevalence of ED increases with aging from 9% in men younger than 40 years to 71% in older men. ED impacts negatively on sexual performance and quality of life (QoL). Low-intensity shockwave therapy (LiSWT) for ED is a regenerative therapy and contrary to other current therapeutic options which are mainly palliative, it restores the erectile mechanism enabling natural or spontaneous erections. LiSWT has found significant usefulness in the treatment of ED with potential to induce angiogenesis and dislodge plaques which will invariably improve blood flood to the penis leading to a lifelong solution to ED with marked improvement in sexual performance. Methodology: This is a prospective randomized study. All patients presenting to andrology clinic with erectile dysfunction were enrolled in the study. Informed consent was obtained. All patients were evaluated to identify the likely etiology and a proforma and standard abridged version of International Index of Erectile Function (IIEF-5) were administered. An Emshock and Smart Tecar 2 in 1 device was used to deliver low intensity shockwave to the penis at 5 different sites and treatment sustained twice a week for 3 weeks to complete a cycle before reassessment with IIEF-5 questionnaire. Data obtained were analyzed using Statistical Package for Social Sciences version 22.0. Results were represented in charts. P value of less than 0.005 was considered statistically significant. Results: Fifty four patients were enrolled in the study. The enrolled patients fell within the age ranges of 34 to 63 years. The identifiable etiology of ED were unknown in 22.22%, diabetes mellitus in 46.30%, hypertension in 18.52% and a combination of hypertension and diabetes in 13%. All patient enrolled for the study had varying degree of abnormal IIEF-5 score. Twelve patients (22.22%) had mild ED, eleven patients (20.37%) had mild to moderate ED, one patient (1.85%) had moderate ED and thirty patients (55.56%) had severe ED. All patients had varying significant improvement in erectile function and IIEF-5 score after the first treatment cycle. Eighteen patients (33.33%) achieved normal erection evidenced by progression to normal IIEF-5 while 36 patients (66.66%) achieved significant progress evidenced by improvement in IIEF-5 score. 4 patients had spontaneous erection that lasted more than 20 minutes during each treatment encounter. No patient had side effect and the patient satisfaction was one hundred percent. Conclusion: LiSWT remains revolutionary as a regenerative therapy for restoration to physiological erectile function possibly possessing unprecedented qualities that can rehabilitate erectile tissue. While results of several studies are variable, one thing that is found across many literatures is the low risk and lack of side effects of LiSWT. Its main benefit is the ability to support and potentially restore erectile function in men with ED without additional pharmacotherapy.
VL - 6
IS - 4
ER -